Intracranial Aneurysms Treatment
Home > Intracranial Aneurysms
Intracranial Aneurysms — Coiling, Flow Diverter & Intrasaccular Devices
What is an intracranial aneurysm?
An intracranial (cerebral) aneurysm is a weakened, bulging area in the wall of a brain artery. Small aneurysms can be monitored, but larger or unstable aneurysms — or those that have bled — may require urgent treatment to prevent rupture or re-bleeding.
Treatment approaches offered
At our neurointerventional unit we offer the full spectrum of minimally invasive endovascular treatments for saccular and wide-neck aneurysms, including:
1. Endovascular coiling (± adjunctive devices)
Endovascular coiling places soft platinum coils into the aneurysm sac via a microcatheter to induce thrombosis and seal the aneurysm off from the circulation.
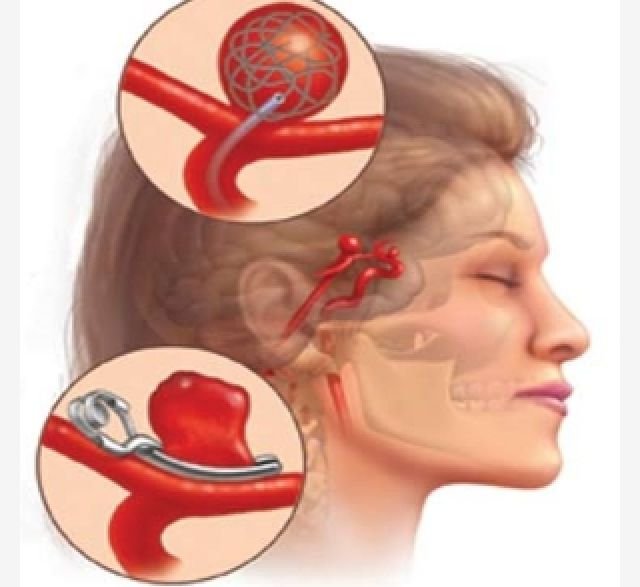
For wide-neck aneurysms, adjunctive techniques such as balloon-assisted coiling or stent-assisted coiling may be used to retain coils in the sac and protect the parent artery. Coiling has a long evidence base and provides good short-term occlusion with low immediate morbidity when performed by experienced teams.
2. Flow-diverter stents
Flow-diverter devices (placed within the parent artery across the aneurysm neck) redirect blood flow away from the aneurysm, promoting progressive thrombosis and vessel remodelling. Flow diversion is especially valuable for certain large, giant, and wide-necked aneurysms that are difficult to treat with coils alone. These devices have demonstrated strong long-term occlusion rates but require careful patient selection and peri-procedural antiplatelet management.
3. Intrasaccular (flow-disruption) devices — e.g., WEB
Intrasaccular flow-disruption devices (such as the Woven EndoBridge — WEB) sit entirely inside the aneurysm neck and sac to disrupt inflow, causing thrombosis while reducing the need for permanent implants in the parent vessel. They are particularly useful for wide-neck bifurcation aneurysms and have shown favorable safety and mid-/long-term occlusion in clinical studies.
How we choose the right option?
Choosing the optimal treatment depends on multiple factors:
Aneurysm size, shape (saccular vs. fusiform), and neck anatomy.
Location (anterior vs. posterior circulation).
Whether the aneurysm has ruptured (subarachnoid hemorrhage) or is unruptured.
Patient age, comorbidities and ability to tolerate dual antiplatelet therapy (required for most flow-diverters and some stents).
Prior treatments or anatomy that may affect access.
In complex cases we may combine approaches (for example, staged coiling followed by flow diversion) to maximize safety and long-term durability. Multidisciplinary discussion (neurointerventionalist, neurosurgeon, neuroradiologist, and critical care team) guides the personalized plan.
What to expect — procedure overview
Pre-procedure evaluation: Detailed imaging (CT angiography / MR angiography / digital subtraction angiography), blood tests and discussion of risks/benefits.
Anesthesia: Procedures are commonly done under general anesthesia or conscious sedation depending on the case.
Endovascular access: A small puncture (usually in the groin or wrist) is used to advance catheters into the head vessels under live X-ray.
Treatment delivery: Coils, flow-diverter stents, or intrasaccular devices are positioned using microcatheters. Adjunctive balloons or stents are used when required.
Immediate imaging: Angiography confirms device position and immediate occlusion status.
Recovery: Patients are monitored in a high-dependency unit; stay length varies (often 24–72 hours for uncomplicated elective cases).